
When Mood and Sleep Begin to Change in Midlife, it can feel less like a “phase” and more like you are slowly losing access to the version of yourself you rely on. You might still be showing up, getting the kids to school, getting through meetings, answering texts, and paying bills. But inside, something feels off: you wake at 3 a.m. with your mind sprinting, or you sleep eight hours and still feel wrung out. Your patience shortens. Your confidence wobbles. Your concentration slips in small, unsettling ways.
In New York City, people often try to push through these shifts the way they push through everything else, one more coffee, one more late night, one more “I’ll deal with it after this quarter.” The problem is that midlife changes can have multiple contributing factors. The same symptoms can be driven by anxiety, depression, hormonal changes (including perimenopause), ADHD that has been masked for decades, medical issues, sleep disorders, grief, burnout, or a combination, medical issues, sleep disorders, grief, burnout, or a combination.
A comprehensive psychiatric evaluation is often the most efficient way to sort through the noise and build a plan that actually fits your life, not a generic checklist.

When Mood and Sleep Begin to Change in Midlife, insomnia can feel like your brain will not “turn off,” especially in a high-demand NYC routine.
When Mood and Sleep Begin to Change in Midlife, what you are really noticing
Most people do not walk into a psychiatrist’s office saying, “I’m depressed,” or “I have anxiety.” They say things like:
- “I’m not sleeping like I used to.”
- “I feel more emotional, and I don’t know why.”
- “I’m irritable with my partner, my team, my kids, everyone.”
- “My memory feels unreliable.”
- “I can’t focus, and it’s scaring me.”
- “I’m fine during the day, then nighttime hits and I spiral.”
A useful analogy: midlife is a time when your internal “settings” may shift, like a phone that suddenly dims its screen, closes _background apps, and drains it_s battery faster. You can still use it, but everything takes more effort, and the glitches feel personal.
The symptoms are real, but they are not always pointing to a single cause.
The most common emotional patterns (without the jargon)
In midlife, mood changes often show up as:
- Anxiety that feels physical: tight chest, stomach flips, jaw tension, a sense that something is about to go wrong.
- Depression that looks like exhaustion: less joy, less motivation, more numbness, more “I don’t care” than “I feel sad.” This presentation is also one of the hardest to distinguish from severe burnout. Our guide on burnout or depression, “a NYC clinician’s clues,” walks through the key differences in plain language.
- Irritability and reactivity: snapping faster, feeling overstimulated, having a shorter fuse with noise, clutter, or conflict.
- A confidence drop: a quiet, constant self-doubt that did not use to run the show.
If you want a deeper read on subtle presentations, the practice’s guide on hidden signs of depression can help you put words to what you might be living. If you’re also unsure whether what you’re feeling is depression or burnout from the relentless pace of NYC life, our newer guide on burnout or depression goes deeper on that distinction.
The sleep changes that tend to worry people most
Midlife sleep complaints often fall into a few buckets:
- Trouble falling asleep: you are tired, but your brain is on.
- Middle-of-the-night waking: the 2 a.m. or 3 a.m. wake-up with racing thoughts.
- Early waking: waking too early and feeling “stuck awake.”
- Lighter, less restorative sleep: you sleep, but you do not recover.
Sleep problems can be a cause, a symptom, or both. That is why it helps to think of sleep as the foundation of the building. When the foundation cracks, every floor above it feels unstable.
For a patient-friendly overview of how sleep supports mental health and what can help, see Can Sleep Heal More Than We Think?.
Why this can happen in midlife, and why it is not “all in your head.”
Midlife often brings a convergence of stressors that do not announce themselves. Instead, they accumulate.
Hormonal shifts, especially perimenopause and menopause
For many women, midlife sleep and mood changes overlap with hormonal transitions. It can feel like your emotional volume knob has been turned up, your sleep has become fragile, and your ability to concentrate has taken a hit.
This does not mean every midlife symptom is hormonal, but it does mean hormones belong in the conversation. If this resonates, you may also want to read Menopause brain fog and memory changes and Managing anxiety, depression, and mood changes during menopause.
For an evidence-based overview of menopause and symptoms, the North American Menopause Society is a reliable resource.
Anxiety and depression that shift shape over time
Midlife anxiety can look less like obvious worry and more like:
- constant mental scanning
- perfectionism that tightens
- panic symptoms that appear “out of nowhere.”
- avoidance that quietly expands (social plans, travel, presentations, even the subway)
Depression can look like going through the motions while feeling disconnected from your own life.
If you want high-quality, plain-language information about these conditions, the National Institute of Mental Health has practical overviews of depression and anxiety disorders.
High-functioning burnout and chronic overload (very NYC)
There is a specific flavor of midlife burnout we see in NYC: the person who is outwardly competent, inwardly depleted. They keep delivering, but everything costs more.
You might recognize it as:
- shorter emotional recovery time
- more “brain static.”
- reduced tolerance for minor problems
- difficulty switching off, even on weekends
Burnout can mimic depression, worsen anxiety, and absolutely wreck sleep.
Attention and concentration changes that are not what you think
When focus slips in midlife, people often fear cognitive decline. Sometimes it is cognitive inefficiency from sleep loss, stress, anxiety, depression, perimenopause, or untreated ADHD that has been compensated for years.
If you are trying to understand whether this is “brain fog” or something more persistent, this guide can be grounding: Brain fog vs cognitive decline: is it just stress or something more?
When Mood and Sleep Begin to Change in Midlife, what a comprehensive psychiatric evaluation actually does
When people hear “evaluation,” they sometimes picture a quick questionnaire and a prescription. A comprehensive psychiatric evaluation should feel very different.
Think of it like detective work, but compassionate. You are not being judged, you are being understood.
A thorough evaluation typically explores:
- Your timeline: what changed first, sleep, mood, focus, energy, appetite, motivation, relationships, work?
- Your context: caregiving, career pressure, grief, trauma history, medical diagnoses, and current medications.
- Your sleep pattern: schedule, awakenings, nightmares, snoring, restless legs, alcohol or cannabis use, and “revenge bedtime procrastination.”
- Your mental load: rumination, panic symptoms, irritability, emotional sensitivity, loss of pleasure.
- Your cognitive concerns: attention, memory, word-finding, processing speed, and decision fatigue.
- Safety: including whether there are any thoughts of self-harm.
If you have ever felt dismissed by a quick screen, it may help to read: Psychiatric evaluation vs online mental health questionnaires.
Sorting the “look-alikes”: a practical map
Many midlife symptoms overlap. This is exactly why a comprehensive evaluation matters.
| What you are experiencing | Could be related to | What an evaluation helps clarify |
|---|---|---|
| Waking at 3 a.m. with racing thoughts | anxiety, hormonal shifts, depression, stress, sleep disorders | what is driving the waking, what keeps it going, and the most targeted treatment |
| Feeling emotionally “thin-skinned.” | burnout, anxiety, hormonal changes, depression | triggers, patterns, and whether therapy, medication, sleep work, or coordination with OB-GYN is indicated |
| Trouble focusing, more mistakes | sleep deprivation, anxiety, depression, ADHD, cognitive inefficiency | whether attention issues are primary (ADHD/executive dysfunction) or secondary to sleep/mood |
| Low motivation, low joy | depression, grief, chronic stress, medical issues | depression subtype signals, functional impairment, and what supports are likely to help |
| Worry about memory or cognitive decline | brain fog, stress, depression, early cognitive change | whether neuropsychological testing is appropriate now or after sleep/mood stabilization |
When neuropsychological testing becomes part of the picture
If changes in concentration or memory are significant, persistent, or professionally risky, neuropsychological testing can provide clarity that talk alone cannot.
A helpful starting point is Neuropsychological testing explained: what it is, who it helps, and what to expect. For some patients, this kind of evaluation provides relief, not because it “labels” you, but because it replaces vague fear with specific information and next steps.
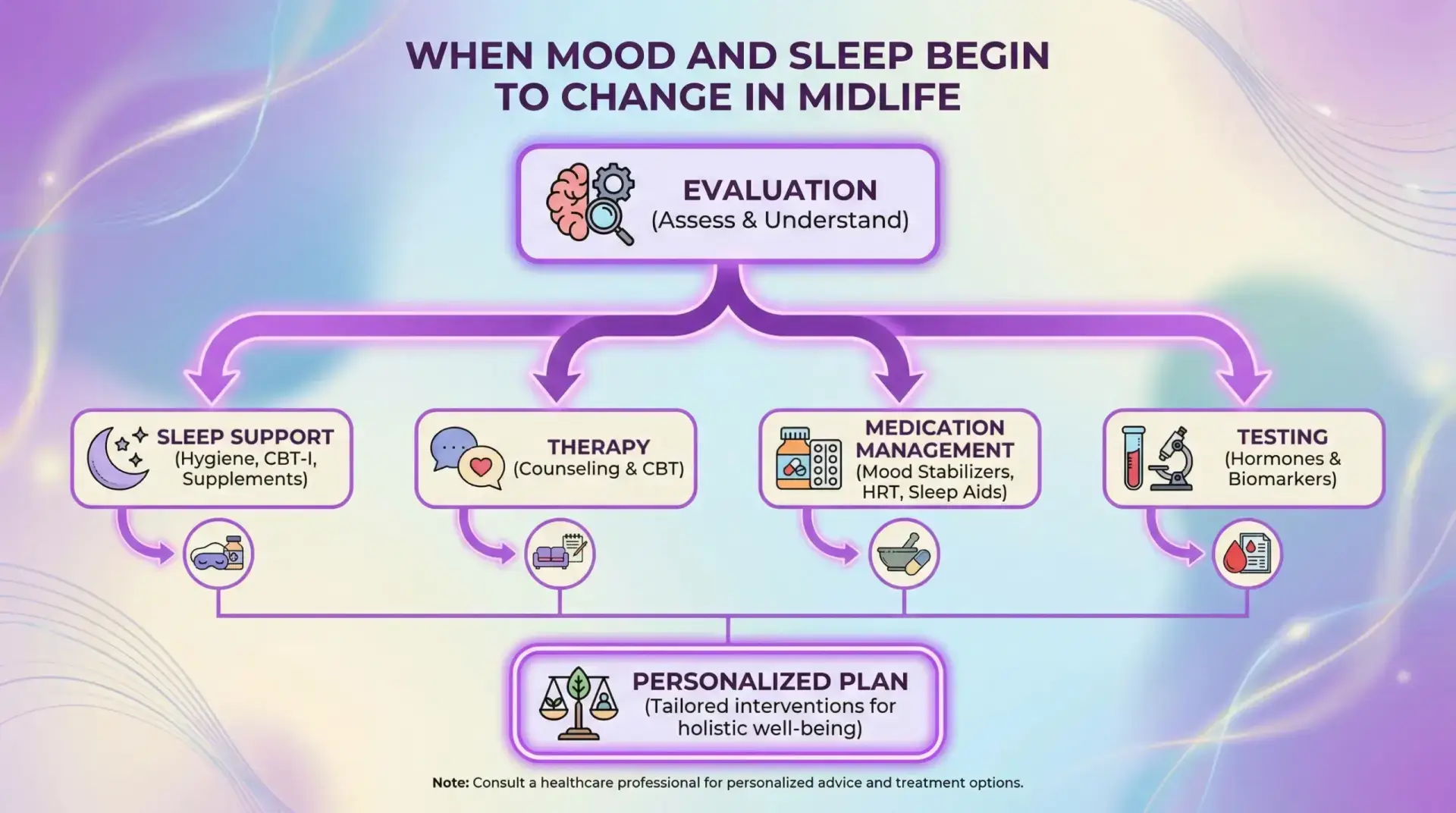
What treatment can look like, when the goal is to feel like yourself again
When Mood and Sleep Begin to Change in Midlife, the best treatment plan usually involves more than a single lever. It is a combination, chosen carefully.
At Dr. Iospa Psychiatry Consulting in Midtown Manhattan (with telepsychiatry across New York, New Jersey, and Florida), care can include therapy, medication management, and specialized testing, coordinated within a multidisciplinary team. The point is to match the approach to your full picture.
Psychotherapy that focuses on real life, not just insight
Evidence-based therapy is not about endlessly analyzing your childhood. It can be practical and skills-based.
- CBT can help you change the thought patterns that spike anxiety at night.
- DBT-informed work can help with emotional overwhelm and reactivity.
- Supportive therapy can help when the stressors are real and heavy, and you need a steadier internal footing.
Medication management that is careful and personalized
Medication is not a personality transplant. When it helps, patients often describe it as “the floor feels steadier” or “my brain finally has traction.”
The right plan depends on many factors, including sleep quality, anxiety patterns, prior medication response, family history, and life stage (including pregnancy planning or postpartum concerns).
If you are considering pregnancy or adjusting medications around fertility and postpartum planning, this resource may be useful: Planning pregnancy while on medication.
Sleep-focused treatment often the fastest relief
When sleep improves, mood and focus often follow. Cognitive Behavioral Therapy for Insomnia (CBT-I) is a structured, evidence-based approach that targets the habits and anxieties that keep insomnia alive.
This is not just “sleep hygiene.” It is a plan.
Cognitive remediation therapy (when “brain stamina” needs rebuilding)
Some patients describe midlife focus issues as mental fatigue, as their brain runs out of battery sooner. When cognitive skills are part of the struggle, cognitive remediation therapy can be an option.
If your team uses video to explain treatment, consider embedding the practice’s internal video hub page about CRT in the body of a related post or service page. You can reference and embed from: Cognitive Remediation 3-Part Series Videos released on YouTube. (This keeps the content on your site while giving visitors a “watch instead of read” option.)
A few “time to get help” signals that matter
Midlife symptoms deserve attention when they are persistent, worsening, or shrinking your life.
Consider reaching out if:
- Sleep problems last more than a few weeks and affect mood or performance.
- You are relying on alcohol, cannabis, or sedatives to fall asleep.
- You are avoiding things you used to handle (subway, meetings, social plans).
- People close to you say, “You don’t seem like yourself.”
- You are scared by your own irritability or emotional swings.
- Concentration issues are affecting work, driving, or safety.
If you are having thoughts of harming yourself, seek immediate help. In the U.S., you can call or text 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room.
Getting care in NYC without making your life harder
New Yorkers often delay care because it feels like one more logistical problem. A practice that offers both in-person Midtown Manhattan appointments and telehealth can reduce friction, especially for:
- executives with unpredictable schedules,
- caregivers balancing parents and children,
- patients who feel too depleted to commute.
Educational disclaimer: This article is for general education and is not medical advice or a diagnosis. If you are concerned about your symptoms, seek an evaluation from a qualified clinician.
Clinically Reviewed by Dr. William Lu, PsyD, Rehabilitation Psychologist, Neuropsychologists