
Menopause brain fog doesn’t feel like what you’d expect. It feels like rereading the same email three times and still not retaining it. Like forgetting a word mid-sentence in a meeting. Like anxiety that showed up without a reason, or a flatness that doesn’t feel like depression but functions like one. If you’ve been writing it off as stress or aging, this is worth reading.
Menopause, brain fog, and the psychiatric symptoms worth discussing
Menopause brain fog often shows up in ordinary moments, not dramatic ones.
The problem is not “in your head”, it is in your context
A pattern we see often in clinical work is that perimenopause does not always create entirely new problems. Instead, it changes the conditions around you.
Here is an analogy many high-functioning New Yorkers relate to. Imagine your brain has been running with a hidden set of “noise-canceling headphones” for years. You were still doing a thousand things, but the background static was softened enough that you could power through. Hormonal shifts can lower that buffering effect. Suddenly, the same workload, the same family logistics, the same emotional labor feel louder and harder to manage.
This is one reason why perimenopause can make symptoms look like:
-
anxiety that came out of nowhere
-
depression that does not feel like sadness
-
a sudden “worsening” of ADHD, even if you were never diagnosed
The National Institute on Aging notes that menopause can bring symptoms like sleep problems, mood changes, and difficulty concentrating, which can overlap with mental health concerns in very real ways (NIA overview).
If you want a deeper dive specifically on cognitive symptoms, you can read our related guide on menopause brain fog and memory changes.
Menopause brain fog that feels like anxiety
Anxiety is not always “worry.” In perimenopause, it can feel more like a body that is stuck on alert.
How patients describe it
People rarely walk in saying, “I’m anxious.” They say:
“I feel jumpy for no reason.”
“My patience is gone, and I hate that version of me.”
“I’m scared I’m slipping at work.”
In NYC, that fear can get specific fast: a presentation in a Midtown conference room, a packed subway when you feel your heart race, a parent-teacher email you cannot bring yourself to answer because your mind is blank.
Why can it be misread?
If a clinician (or an online questionnaire) looks only at symptoms on paper, menopause brain fog plus sleep disruption can resemble generalized anxiety or panic. But the timeline matters. Many women can point to a window when things shifted: cycles became irregular, sleep changed, patience thinned, and focus started to cost more effort.
If panic symptoms are part of your picture, our team also wrote a patient-centered explainer on anxiety and panic attacks.
What is worth discussing in an appointment
Try bringing concrete examples rather than labels:
-
When did the “mental static” start?
-
Does it spike before your period, or does it spike as your cycle becomes unpredictable?
-
Is it paired with insomnia (especially waking at 3 a.m. with a racing mind)?
-
Are you avoiding things you used to do easily (driving, presentations, social plans)?
Those details help your clinician see whether the primary driver is anxiety, hormone-related sleep disruption, ADHD-like executive overload, depression, or a combination.
Menopause brain fog that looks like depression, even if you still function
Depression in midlife is often quiet. Many people keep showing up. They answer Slack messages. They get kids fed. They do the thing.
But inside, it feels like moving through wet cement.
The “hidden” depression pattern
Some women describe it as emotional flattening, less joy, less spark, more irritation, less tolerance for noise, and a reduced ability to recover from stress. Others describe shame: “I should be grateful. Nothing is wrong. Why do I feel like this?”
The National Institute of Mental Health describes depression as involving changes in mood, interest, energy, sleep, and thinking, not only sadness (NIMH overview). That broader definition matters in perimenopause, where the presenting complaint might be “I can’t think” or “I’m failing,” not “I’m depressed.”
If you are wondering whether what you feel is depression or burnout, you may also find it helpful to read about depression treatment in Midtown NYC, how to spot the hidden signs.
Menopause brain fog that looks like ADHD, and the “coping buffer” that disappears
This is the moment many high-achieving women tell us they finally feel “caught.” Not because they became less capable, but because the strategies that worked for decades stop working.
If you have always relied on urgency, adrenaline, perfectionism, or last-minute sprints to get things done, perimenopause can make that system crash. You may still be smart and driven, but your brain no longer cooperates the same way.
Signs women often miss
In adult women, ADHD can show up as:
-
chronic overwhelm, even when life looks “together.”
-
intense procrastination paired with high standards
-
losing track of time, tasks, or conversational threads
-
emotional reactivity that feels out of proportion
Perimenopause can amplify all of this. Sleep disruption alone can mimic ADHD symptoms, and hormone shifts can change how resilient your attention feels.
If this resonates, you might relate to our article on how ADHD looks different in professional women. The overlap is not theoretical, it is what many patients live.
The clinical risk
Without factoring in the hormonal context, a clinician might misread the situation in either direction:
-
Assuming “it’s just hormones” and missing depression, anxiety, or lifelong ADHD
-
Treating anxiety or depression without noticing that executive function is the core impairment
A careful assessment should make room for both truths.
When postpartum is the “other” hormonal window that can mimic psychiatric illness
Perimenopause gets more attention lately, but postpartum is another major transition where symptoms can look psychiatric, cognitive, or both.
Some people expect postpartum depression to feel like sadness. Instead, they feel:
-
wired but exhausted
-
scared of making a mistake
-
unable to sleep even when the baby sleeps
-
emotionally flooded, then numb
The American College of Obstetricians and Gynecologists describes postpartum depression as common and treatable, and encourages reaching out rather than white-knuckling through it (ACOG FAQ).
Why mention postpartum in a menopause brain fog article? Because the pattern can rhyme.
Many women say, “I felt like this after my first baby, and now it’s back.” For some, that is a clue that their nervous system is sensitive to hormonal shifts and that targeted support is worth seeking early, not after months of feeling unrecognizable.
What to bring to a menopause-informed psychiatric visit, so you feel understood fast
A good first visit should not feel like you are defending your reality. It should feel like someone is helping you organize the story.
A simple tracking framework
Think of your symptoms as three layers: brain, body, and life.
-
Brain: focus, word-finding, decision fatigue, short-term memory slips
-
Body: sleep quality, night sweats/hot flashes, heart racing, appetite changes
-
Life: work stress, caregiving load, relationship tension, alcohol/caffeine changes
Questions you can ask
-
“Could sleep be driving this, and what are our options to address it?”
-
“How do we tell the difference between ADHD, anxiety, and menopause-related cognitive inefficiency?”
-
“If we try therapy or medication, what would ‘working’ look like in my daily life?”
-
“Should we consider formal testing to get a baseline?”
If you are feeling mood symptoms and want a menopause-specific overview, you can also read Managing Anxiety, depression, and mood changes during menopause.
When neuropsychological testing is the right next step, and when it is not
In our Midtown Manhattan practice, one of the most relieving moments for patients is when we stop guessing.
What testing can clarify
If your biggest fear is cognitive decline, or if focus problems have become professionally risky, a neuropsychological evaluation can help separate:
-
attention and executive function issues
-
memory encoding versus retrieval issues
-
mood-driven cognitive slowdown
-
stress and sleep effects
It can also provide a baseline so you are not evaluating yourself only through a lens of fear.
If you are curious what that process actually involves, we explain it in plain language here: What is a neuropsychological evaluation?
Treatment is not only medication
A menopause brain fog plan might include psychotherapy (CBT, DBT, or supportive therapy), medication management when appropriate, sleep-focused interventions, and cognitive skills work.
If you learn best visually, consider embedding the practice’s short video content in this section of the page, especially our CRT series announcement, designed for patients who want to understand how targeted cognitive work can improve attention and mental flexibility: Cognitive Remediation Therapy (CRT) video series.
Red flags that deserve faster support
Most menopause brain fog is not dangerous, but some symptoms should move you from “I’ll wait it out” to “I want help now.”
Seek urgent support if you are having thoughts of harming yourself, you cannot safely care for yourself or a baby, you are using substances to get through the day, or your anxiety is producing repeated panic episodes and avoidance that is shrinking your life. If you are in immediate danger, call 911. In the U.S., you can also call or text 988 for the Suicide & Crisis Lifeline.
Frequently Asked Questions
Is menopause brain fog the same as dementia? No. Menopause brain fog is often described as slowed thinking, distractibility, or word-finding trouble, especially with poor sleep. Dementia involves a progressive decline that interferes with daily functioning in a different way. If you are worried, a structured evaluation can clarify what is going on.
Why does menopause brain fog feel like anxiety? Because when concentration drops, and sleep gets lighter, your brain can interpret normal demands as threats. You may feel keyed up, irritable, or physically restless, even if you are not “worrying” all day.
Can perimenopause trigger depression even if I have never been depressed before? It can. Hormonal shifts, sleep disruption, stress load, and life transitions often converge in midlife. Getting help early is not overreacting; it is preventive care.
How do I know if it is ADHD or menopause brain fog? The timeline and your life history matter. ADHD typically has roots earlier in life, even if it was masked by structure or perfectionism. Menopausal brain fog may be more closely linked to cycle changes and sleep disruption. Many people have both, and a careful evaluation can sort out priorities.
What kind of clinician should I see in NYC? Many patients do best with coordinated care, psychiatry for diagnosis and medication management when appropriate, psychotherapy for skills and emotional support, and neuropsychological testing when cognitive questions are central. Telepsychiatry can work well if scheduling and commuting are barriers.
A next step that is calm, practical, and personalized
If you are navigating menopause brain fog, postpartum mood changes, or a sudden spike in anxiety, depression, or attention symptoms, you deserve an assessment that accounts for your full context, hormones, sleep, stress, and cognitive load.
Dr. Iospa Psychiatry Consulting provides comprehensive psychiatric and psychological care in Midtown Manhattan and via telehealth across New York. Our multidisciplinary team offers psychotherapy, medication management, and neuropsychological testing when needed.
-
Explore services and request an appointment: Comprehensive Psychiatric Services in NYC
-
If cognitive concerns are front and center: What is a neuropsychological evaluation?
Educational disclaimer: This article is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified clinician. If you think you may be experiencing a medical or psychiatric emergency, call 911 or go to the nearest emergency room. In the U.S., you can also call or text 988 for immediate support.
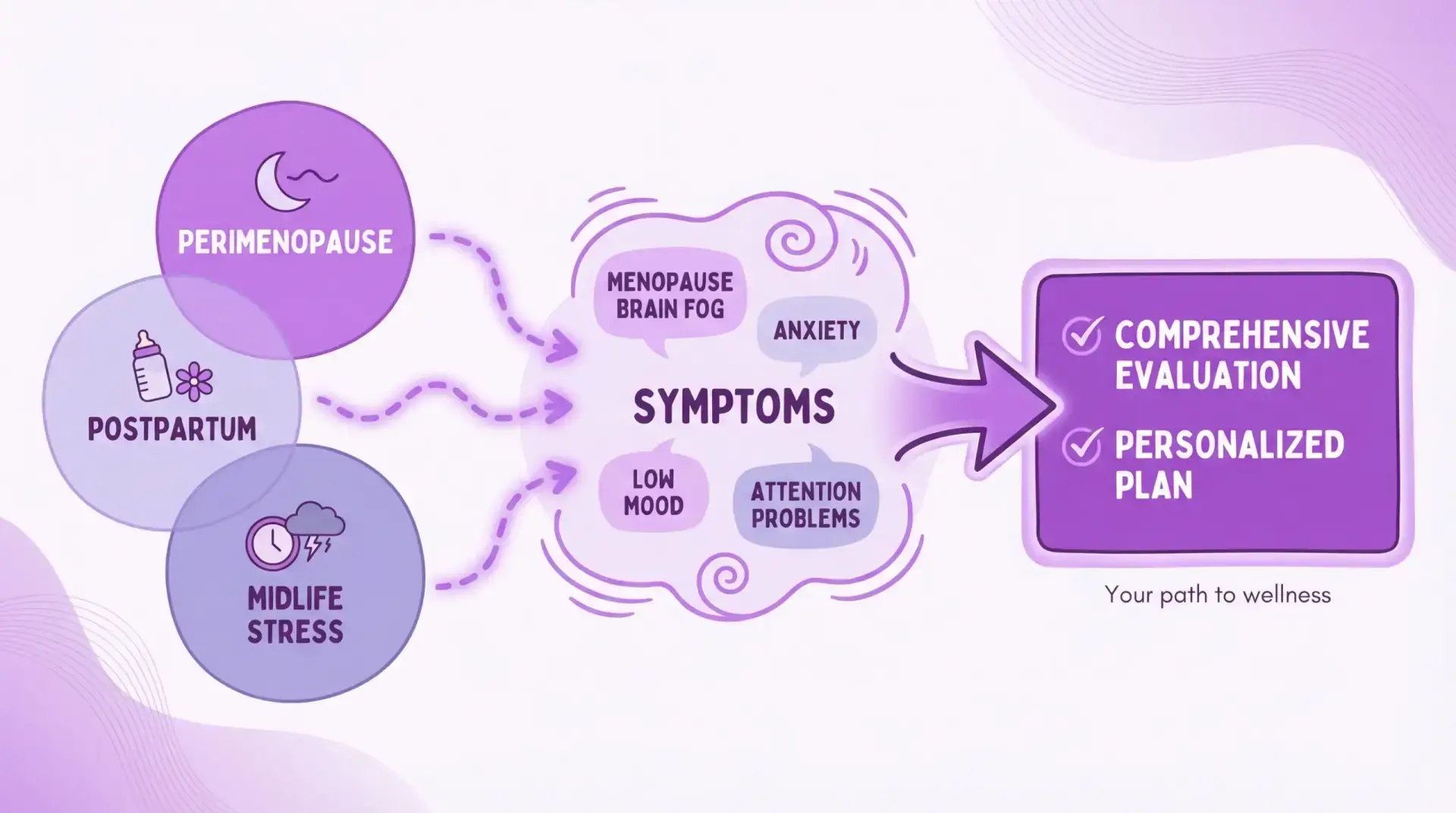
Hormonal transitions and life stress can overlap; a comprehensive evaluation helps sort what is driving your symptoms.