
Sleep disruptions are stressful for any family. But when a child starts having vivid nightmares, screaming episodes that look like a “panic attack,” or a sudden fear of going to bed, it can quickly become a whole-house problem: missed school, exhausted parents, and worsening anxiety the next day.
In NYC, we also see how packed schedules, long commutes, selective school pressure, and late-night screens amplify sleep anxiety in children and teens. The good news is that many sleep problems respond well to targeted, evidence-based care once you identify what’s actually happening at night.
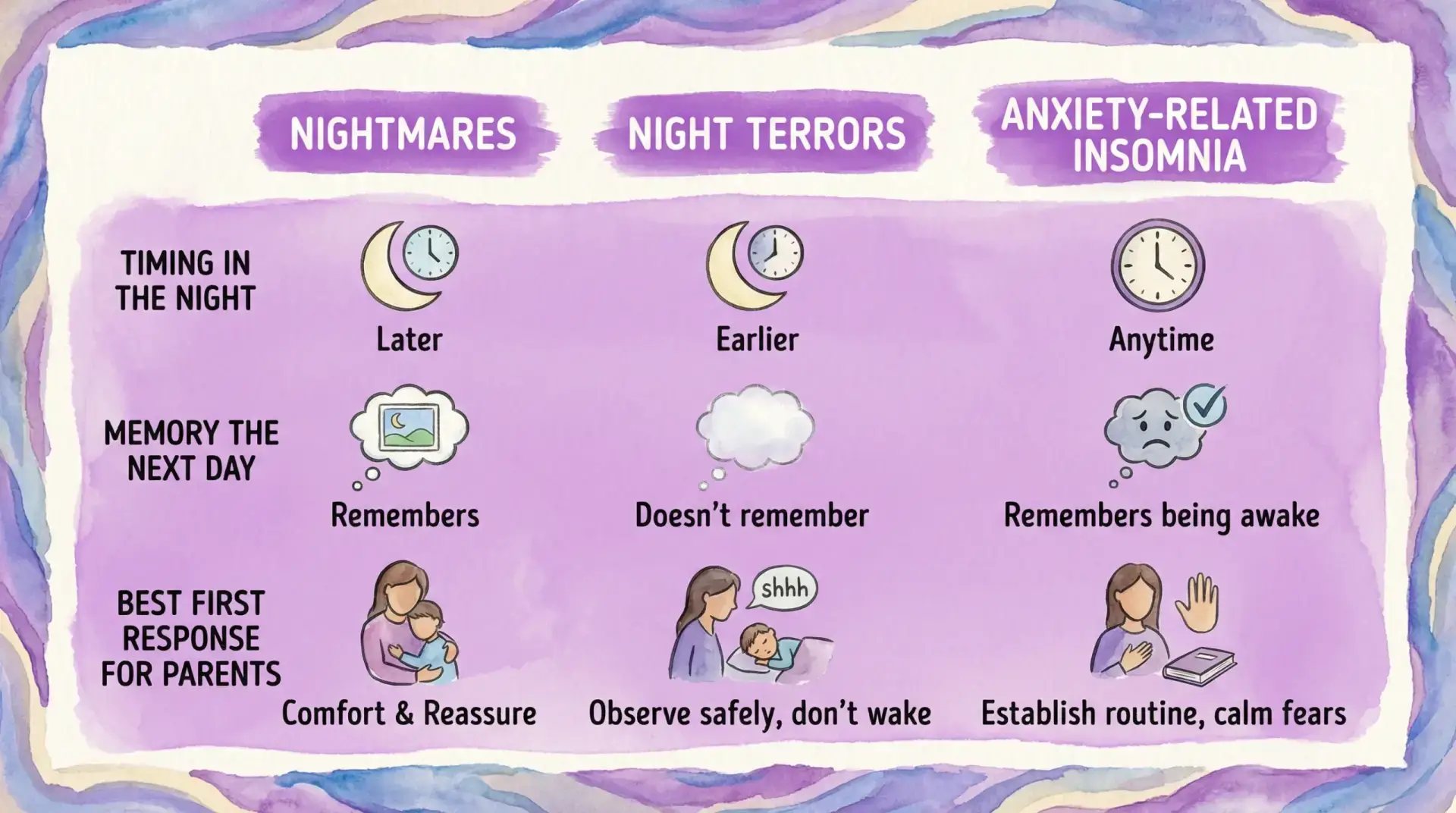
Nightmares vs. night terrors vs. anxiety-driven insomnia (why the distinction matters)
Families often use “nightmares” as a catch-all. Clinically, these experiences can be very different, and treatment changes depending on which pattern fits.
| What it looks like at night | Most likely category | Typical timing | Does the child remember it? | Common daytime clues |
|---|---|---|---|---|
| Child wakes fully, scared, can describe a dream | Nightmare | Second half of the night | Yes | Fear of sleep, reassurance-seeking |
| Child screams, looks terrified, hard to wake, may thrash | Night terror (sleep terror) | First third of the night | No or very limited | Child seems “fine” in the morning, parents are traumatized |
| Child can’t fall asleep because of “what if” worries | Anxiety-related insomnia | Bedtime and sleep onset | N/A | Perfectionism, separation worries, somatic complaints |
| Child wakes with racing heart, shortness of breath | Nocturnal panic or anxiety surge | Any time | Sometimes | Panic symptoms, avoidance, anticipatory anxiety |
| Recurrent nightmares after a scary event | Trauma-linked nightmares | Variable | Often yes | Hypervigilance, irritability, regression |
Academic pediatric centers note that night terrors are usually a non-REM parasomnia and are often more distressing for the observer than for the child the next day. For an overview of typical patterns, see Boston Children’s Hospital’s explanation of night terrors.
When sleep issues cross the line into “needs treatment”
Occasional nightmares are part of development. Treatment becomes important when sleep disruption starts affecting safety, mood, school, or family functioning.
Consider a Midtown Manhattan sleep evaluation (or an NYC telehealth child psychiatrist consult) if you notice:
- Nightmares or night terrors happening weekly (or clustering for weeks)
- Bedtime anxiety that escalates into tears, panic, or refusal to sleep alone
- Daytime impairment: irritability, concentration problems, falling grades, more conflicts
- New symptoms after a stressor (bullying, family change, accident, medical event), suggesting nightmares trauma child patterns
- Sleep deprivation worsening attention and impulse control (often mistaken for “behavior problems”)
- Snoring, breathing pauses, restless sleep, or unusual movements (these warrant a medical sleep or pediatric evaluation)
If your child expresses self-harm thoughts, seek urgent help immediately (in the U.S., you can call or text 988).
Sleep anxiety in children: what it often looks like in NYC homes
Sleep anxiety in children isn’t always “I’m anxious.” It often shows up as:
- Endless bedtime questions (“What if I can’t sleep?” “What if something happens?”)
- Repeated trips out of bed for water, bathroom, checking noises
- Needing a parent to stay until they fall asleep (and escalating when you try to leave)
- Stomachaches or headaches that peak at bedtime
- “Sunday night insomnia” tied to school pressure
A helpful starting point is separating two drivers:
- Fear-based driver (scary images, separation fears, trauma reminders)
- Performance driver (“I have to sleep or tomorrow will be ruined”), which can become a self-fulfilling cycle
How ADHD and sleep problems feed each other
Parents are often told, “It’s just ADHD,” or, “It’s just anxiety.” In real life, sleep and attention problems interact.
Sleep loss can intensify sleep problems and ADHD symptoms such as distractibility, emotional reactivity, and poor impulse control. Meanwhile, ADHD can make bedtime harder because transitions, winding down, and shutting off stimulation are genuinely challenging.
If you suspect attention issues alongside sleep, a comprehensive evaluation can help clarify what’s primary and what’s secondary. Depending on the question, that may include psychiatric assessment plus testing, such as private ADHD testing in NYC or a school-focused evaluation for accommodations.
For students seeking documentation, psychoeducational testing may be appropriate, especially when insomnia, anxiety, and academic performance collide. Learn more in how psychoeducational testing can help.
What parents can do tonight: “bedtime anxiety help” that doesn’t backfire
Many well-intentioned strategies accidentally reinforce anxiety (for example, unlimited reassurance or negotiating bedtime for hours). These steps are a better first line:
Keep the response boring, consistent, and brief
For nightmares: comfort, orient to the present, then return to bed.
For night terrors: prioritize safety (prevent injury), keep lights low, and avoid trying to fully wake the child.
Shift reassurance into a plan
Instead of “Nothing bad will happen,” try: “If your brain sends a scary story, here’s what we do: three slow breaths, hug, back to bed.”
Protect sleep drive
Late naps, sleeping in, and long “recovery mornings” can keep the cycle going. The CDC’s sleep duration guidance can help you sanity-check age-appropriate totals (see CDC sleep recommendations).
Be intentional about screens and late-night engagement
If your teen is up late gaming or doomscrolling, it’s not just “bad habits.” Many digital products are built to maximize continuous engagement through real-time feedback loops and rewards. Even outside gaming, you can see how “always-on” design is positioned as a feature in other industries, for example in real-time analytics platforms that optimize ongoing user activity. For sleep, the takeaway is practical: create a predictable cut-off time, move devices out of the bedroom, and expect pushback at first.
Evidence-based treatment options (and what “child insomnia treatment NYC” can look like)
The right care depends on whether the main problem is insomnia, anxiety, trauma, ADHD-related dysregulation, or a combination.
1) CBT-I and behavioral sleep strategies (often first-line)
Cognitive Behavioral Therapy for Insomnia (CBT-I) is widely recognized as an effective, structured approach for insomnia, including when anxiety is part of the cycle. It focuses on sleep scheduling, reducing sleep-related fear, and strengthening the bed-sleep association.
If you want a clinic-level overview of why sleep treatment can improve mental health symptoms, see Can Sleep Heal More Than We Think?.
2) Therapy for anxiety, panic, or trauma
When bedtime fear is part of a broader anxiety pattern, CBT (and sometimes DBT skills for emotion regulation) can reduce anticipatory anxiety and physiological arousal.
If your child’s sleep struggles are one piece of a larger anxiety picture, you may find it helpful to review childhood anxiety red flags and how families can respond without reinforcing avoidance.
For trauma-linked nightmares, treatment may include trauma-focused therapy and, in some cases, nightmare-specific approaches such as Imagery Rehearsal Therapy (IRT), guided by a clinician.
3) Medication management (when appropriate, and carefully)
For some children and teens, medication can play a role, particularly when insomnia is driven by moderate-to-severe anxiety or depression, or when ADHD treatment needs adjustment.
It’s also worth noting that many families ask about melatonin. The NIH Office of Dietary Supplements summarizes evidence and safety considerations in its melatonin fact sheet. Because supplements are not regulated like prescription medications, dosing and purity can vary, so it’s best to discuss with a clinician who can weigh benefits, risks, and the real target problem.
4) Testing when sleep issues overlap with learning, attention, or cognition
Sleep problems can mimic ADHD, worsen executive function, and affect memory. In teens, chronic insomnia can look like “laziness” or “defiance” when it’s actually fatigue and diminished self-control.
If your child needs clarity for school planning, accommodations, or differential diagnosis, your clinician may recommend neuropsychological or psychoeducational assessment. Start here:
Teen insomnia: when it’s time to involve a specialist
A teen insomnia psychiatrist NYC search often comes after months (or years) of escalating patterns: 2 a.m. bedtimes, daytime sleeping, missed first periods, panic about grades, and stimulant or caffeine patterns that complicate sleep further.
Treatment is especially important when:
- The sleep schedule has shifted dramatically (possible delayed sleep phase)
- Anxiety, depression, or panic symptoms are present
- There’s significant impairment (attendance, grades, social withdrawal)
- The teen is using substances or high doses of caffeine to cope
A specialized evaluation helps separate biology (circadian rhythm), behavior (reinforcement patterns), and mental health drivers so treatment targets the right mechanism.

What to expect from a Midtown Manhattan sleep evaluation at our practice
At Dr. Iospa Psychiatry Consulting, our goal is not to “sedate” sleep problems, it’s to understand and treat what’s maintaining them.
A pediatric sleep mental health NYC evaluation commonly includes:
- A detailed sleep history (timing, awakenings, nightmares vs night terrors)
- Screening for anxiety, panic, depression, ADHD, and trauma exposure
- Review of medications and supplements, including timing and side effects
- School and family context (stress load, accommodations, schedule constraints)
- A treatment plan that may combine psychotherapy, skills coaching, and medication management when indicated
Care is available in Midtown Manhattan and via telehealth for New York patients, which can be especially helpful for families coordinating school and work schedules.
We also work collaboratively across disciplines. If cognitive or attention concerns are part of the picture, you may benefit from consultation with our neuropsychology team, including Dr. Dana Haywood. You can explore her cognitive-focused work and resources through our site, including the Cognitive Remediation Therapy (CRT) video series with Dr. Dana Haywood.
Frequently Asked Questions
How can I tell if my child is having nightmares or night terrors? Nightmares usually fully wake a child and are remembered. Night terrors often happen earlier in the night, the child may scream or thrash, is difficult to wake, and typically doesn’t remember in the morning.
Can anxiety cause insomnia in kids even if they seem fine during the day? Yes. Many children “hold it together” at school and unravel at bedtime. Sleep anxiety in children often shows up as reassurance-seeking, frequent checks, and fear of being alone rather than obvious daytime worry.
Do sleep problems worsen ADHD symptoms? Often, yes. Poor sleep can worsen attention, impulse control, and emotional regulation, which can look like ADHD or amplify existing ADHD. A comprehensive assessment can clarify what’s driving what.
Is melatonin safe for children? Melatonin may be appropriate in some situations, but it should be discussed with a clinician because dosing and product quality vary and it may not address the root cause. The NIH Office of Dietary Supplements provides a detailed overview in its melatonin fact sheet.
When should I seek child insomnia treatment in NYC? Seek care when sleep problems are frequent, persistent, or impairing (school, mood, family functioning), or when nightmares, night terrors, or bedtime anxiety are escalating. Early treatment can prevent the cycle from becoming chronic.
Next step: get a targeted plan instead of guessing
If you’re looking for child insomnia treatment NYC families can rely on, Dr. Iospa Psychiatry Consulting offers comprehensive, personalized care in Midtown Manhattan and via telehealth in New York. We help families distinguish nightmares from night terrors, identify anxiety or ADHD overlap, and build an evidence-based plan that supports sleep and daytime functioning.
Explore our practice at Comprehensive Psychiatric Services in NYC and schedule a consultation to discuss a Midtown Manhattan sleep evaluation or NYC telehealth options.